
A complete IVF cycle takes approximately 4-6 weeks from the start of stimulation to embryo transfer.
Including pre-cycle preparation and testing, most patients should plan for 2-3 months from first consultation to pregnancy test. If you are doing IVF with preimplantation genetic testing (PGT), add another 2-4 weeks for biopsy results.
That’s the short answer. The longer answer – the one that helps you actually prepare – is what this guide is for.
It walks you through each stage exactly as we explain it in our clinic: clinically precise, practically grounded, and always honest about what to expect.
Key Takeaways
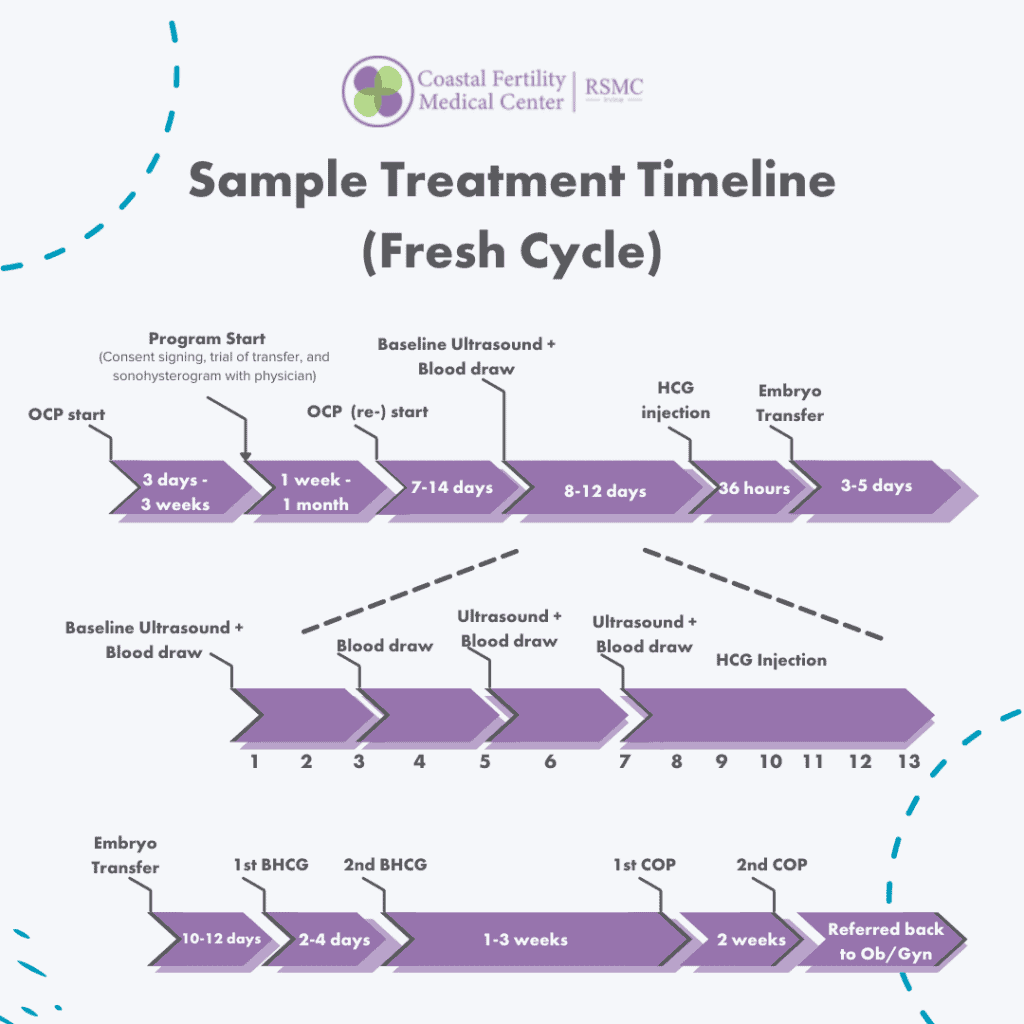
IVF Timeline at a Glance
The table below shows the full IVF process timeline from first consultation to pregnancy test.
Every phase has a typical duration – though your personalised calendar will depend on your protocol, your body’s response, and whether you’re doing a fresh or frozen transfer.
If you are proceeding with a frozen embryo transfer (FET) rather than a fresh transfer, add approximately 4–6 weeks for a separate FET cycle. If you are doing IVF with PGT, add 2–4 weeks for genetic biopsy results before transfer.
Phase 1: Initial Consultation and Pre-Cycle Testing (2–4 weeks)
Phase 2: Pre-Cycle Preparation (3-7 weeks)
Phase 3: Ovarian Stimulation (8-12 days)
Phase 4: The Trigger Shot and Egg Retrieval (36 hours + 1 day)
Phase 5: Fertilisation and Embryo Development (3–6 days)
Phase 6: Embryo Transfer (1 day)
Phase 7: Post-Transfer Monitoring and Pregnancy Confirmation (6-10 weeks)
What Affects Your IVF Timeline?
What Affects Your IVF Timeline?
Sample IVF Timeline Calendar
IVF Timeline With PGT (Preimplantation Genetic Testing)
How Many IVF Cycles Might You Need?
Thinking in Cumulative Metrics
Insurance Coverage for IVF in California
What SB 729 covers (for eligible plans):
Which plans are covered:
Key exemptions — plans NOT covered by SB 729:
Frequently Asked Questions
Julianna Nikolic
Chief Strategy Officer Julianna Nikolic leads strategic initiatives, focusing on growth, innovation, and patient-centered solutions in the reproductive sciences sector. With 26+ years of management experience and a strong entrepreneurial background, she brings deep expertise to advancing reproductive healthcare.
![]()
